
On HRT & Approaching 60?
"There is no arbitrary limit for duration of HRT use"
〰️
"There is no arbitrary limit for duration of HRT use" 〰️
Over the last month or so I've had a number of patients and friends express concern that their GP has talked about stopping their MHT (menopausal hormone therapy/HRT) as they are at, or are approaching age 60.
This information is outdated and incorrect.
I have therefore pulled together the up-to-date guidelines from reputable websites for you to take to your GP.
Guidelines as at February 2026
NICE = National Institute for Health and Care Excellence (England & Wales) provide consistent high quality care across NHS and private sector. The NICE guidelines are world renowned and used across multiple countries.
SIGN = Scottish Intercollegiate Guidelines Network & the Scottish Medicines Consortium are the equivalent in Scotland (but they pretty much follow the NICE guidelines.
From the NICE Guidelines (Feb 2026) :
Advise that: HRT should be continued for as long as benefits of symptom control and improved quality of life outweigh any risks — there is no arbitrary limit for duration of HRT use.
To find that particular paragraph takes a bit of hard work….
Once you open the above link, scroll down to the heading, “How Should I Manage Menopausal Symptoms with Hormonal Replacement Therapy”, then scroll down to the last paragraph before the heading, “Risks of HRT”
Scotland Specific advice from NHS Lothian (Feb 2026) :
6. Duration of use of systemic HRT
6.1 How long can HRT be used for?
Use of HRT should be reviewed on an annual basis. HRT-associated health risks (particularly breast cancer) increase with age and duration of use. However, there are also HRT-associated health benefits and there is no maximum age or duration of use and if an informed individual without medical contraindications considers that HRT benefits outweigh risks for them, continuation can be supported.
https://apps.nhslothian.scot/refhelp/guidelines/sexualreprohealth/menopause/menopause-and-hrt
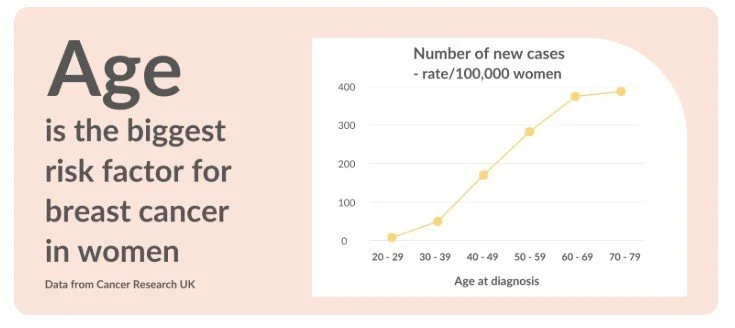
I feel it is worthwhile noting that yes, risk of breast cancer does increase with age - but as yet, there is no explanation as to why this happens see graph below.
Also, in the early 2000’s when the majority of women stopped taking HRT due to the flawed information from the WHI study, the incidence of breast cancer continued to rise.
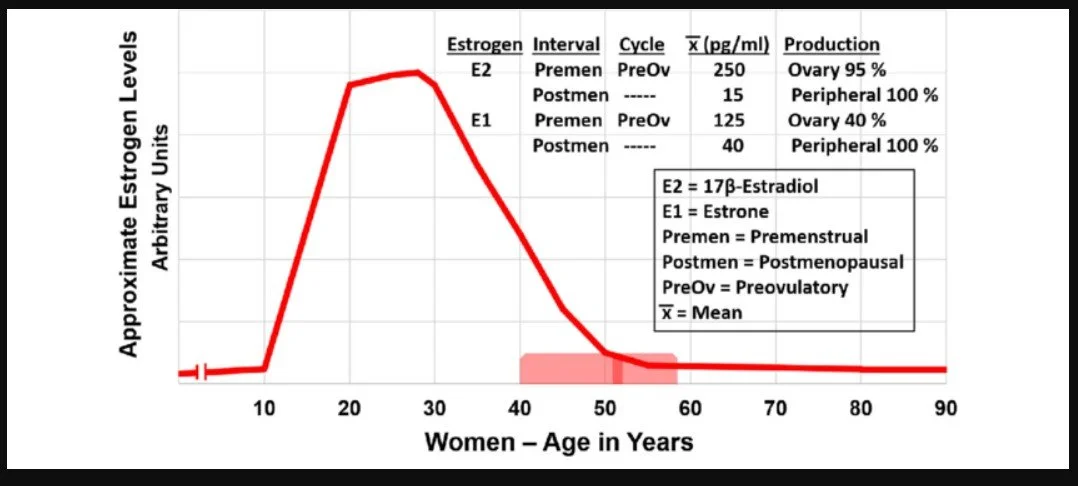
And, as a female ages, her levels of oestrogen drop significantly, so trying to correlate the ‘oestrogen causes breast cancer’ theory becomes harder to explain.
Talking of breast cancer....
The most recent consensus statement from The British Menopause Society on the subject states;
The risk of breast cancer diagnosis associated with hormone replacement therapy is often assumed by health care professionals and the lay public alike, to be very high, which may adversely influence decisions about its initiation and continuance. (primarily due to the flawed WHI study in the early 2000's JMc.)
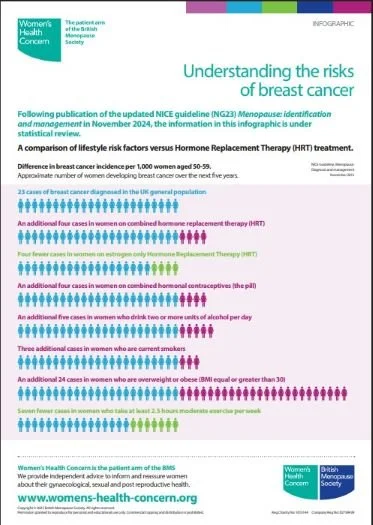
Risk associated with HRT (including past users) is less than other lifestyle risk factors for breast cancer. (see image below JMc.)
There is no additive effect of HRT exposure in women at elevated personal risk due to a family history or high-risk benign breast condition
You can read the key points of the consensus statement here:
https://thebms.org.uk/publications/consensus-statements/risks-and-benefits-of-hrt-before-and-after-a-breast-cancer-diagnosis/
Sadly Scottish guidelines add to the confusion as they state:
Family history of breast cancer (unlike personal history of breast cancer) is not a contraindication to HRT. Using combined HRT does, however, increase risk of breast cancer and this may be additional to inherited increased risk.
However, it does go on to say:
- When considering HRT formulation, people with a family history of breast cancer might choose to use HRT that contains micronised progesterone or dydrogesterone as the progestogen component. These preparations appear to confer a smaller increase in breast cancer risk (in the general population) than combined HRT containing some other synthetic progestogens
NB. This was compiled using the old style oral conjugated equine estrogens CEE (from pregnant mares) and progestogens, not transdermal estradiol & micronised progesterone.
Sadly, any woman in the UK has a 1 in 7 chance of developing breast cancer over her lifetime.
Whilst there are risk factors that we can control there are others that we cannot but, as at the time of writing, the world has yet to work out a definitive reason why some people develop any cancers whilst others don't.
We will all know a 90 year old lady who smoked 60 a day and never got lung cancer. A neighbour of mine, for example!
This Magic Age of 60!
The old advice was that women would not need MHT by the time they were 60, plus as we age the risk of cardiovascular disease and blood clots rises. This is potentially due to the fact that oestrogen is known to keep our blood vessels healthy and pliable and as our levels decline, our risks ‘catch-up’ to be inline with those of males - usually approx 10 years after menopause.
G.Ps. who are not reading their guidelines will therefore still have this magic age of 60 as the date when we’re to be taken off it.
However, the current guideline states that if we choose to continue to take MHT after age 60, we should be taking estrogen transdermally, not orally:
- People who continue HRT intake over the age of 60 should be advised to have estradiol administered transdermally.
And from the NHS Lothian website:
4.2.1 Should I prescribe HRT containing oral or transdermal estradiol?
HRT containing transdermal estradiol (estradiol patches, gel or spray) appears not to confer an increased risk of VTE or stroke in the general population whereas HRT containing oral estradiol is associated with increased risk of thrombosis.
HRT containing transdermal (rather than oral) estradiol is therefore particularly recommended for individuals aged over 60 years and those with risk factors for venous thromboembolism or cardiovascular disease (eg BMI>30, smoker, migraine with aura, diabetes, cancer treatment, reduced mobility).
Transdermal estradiol is also preferable for people taking thyroxine and those with liver/gallstone disease. Route of estradiol administration does not appear to affect breast cancer risk.
Why Is Transdermal Better than Oral tablets?
Our clotting agents are produced by the liver, a vital process for stemming blood flow should we injure ourselves.
Taking oestrogen orally (a tablet) means that it has its' 1st pass through the liver.
Taking oestrogen transdermally means that the hormone is absorbed directly into the bloodstream through the skin, thereby avoiding the liver altogether and avoiding promotion of clotting agents.
As oral oestrogen tablets have been around for much longer, my guess is that the reason they are still offered as frequently - at least in NHS Lothian they can be, is that they are much cheaper than the newer forms.
And remember, oestrogen in and of itself does not cause breast cancer. If it did then puberty and pregnancy would be risk factors and they're not.
Also, the contraceptive pill can contain up to 10X more hormone than HRT - contraception needs to be way more powerful to stop pregnancy, whilst HRT is only supplementing our hormone levels. (& how easy is it for 16 year olds to be given the contraceptive pill and then be on it for years)
The rules change if a female develops an oestrogen positive cancer but I won't go into that for now. That's a whole other ball game.
I Need a Lie Down Now!
If you've read this far - well done!
This has been a lot. And yes, it is confusing.
Remember, if you struggle with all of this info, you can book a Menomate appointment with me, usually via zoom or whatsapp video chat. Email me to arrange.
Summary
Don't let anyone tell you that you should or should not be taking a medication of any kind, based on their own personal assumptions, without using the most up to date guidance. GP or not!
Advocate for yourself by looking up reputable websites such as the ones listed above
If you are being told that you are not 'allowed' HRT after 60, please print off the links above and take to your GP (information correct as of 16th Feb 2026)
GPs are exhausted. You're aiming to help them, not fight with them.
You are allowed to seek a 2nd opinion.