
Reassurance & Rehab
The importance of reassurance and education in rehab.
How Did We Get From this To This In Only 1 Session?

27th Jan 2026

5th Feb 2026
This patient's improvement in a such a short space of time was brilliant - a real gold star student!
What was the secret?
This lady had tripped over and fallen in mid-October 2025, landing on her right arm which resulted in a fracture at the 'top' of her upper arm bone - the humerus.
At A & E she was x-rayed, given a sheet of shoulder rehab exercises - entitled Proximal Humerus Fracture - and sent home.
She had no further physio nor medical appointments.
At her request, "my arm felt so vulnerable", she was given a rudimentary sling to use. She was not going to be given one, even though the above mentioned hand-out states that she would be. So she’s now confused as well as in pain.
Understandably, she was unable to perform the exercises given at the time - her arm was broken - but there was no follow up appointment to see how she was healing or if she was doing the exercises correctly.
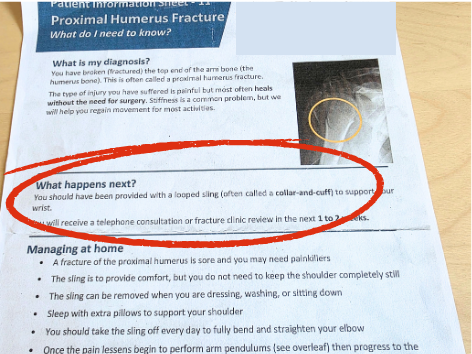
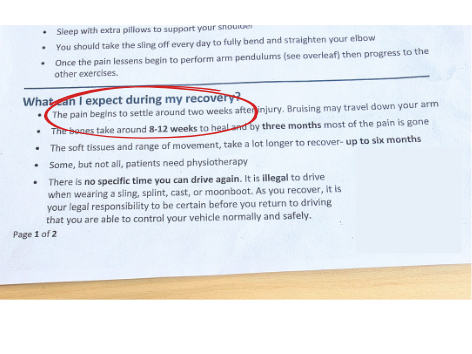
The phrase, “the pain begins to settle around 2 weeks after injury” is somewhat vague, although I know what it means it can confuse the patient. And, when the patient tries the exercises and they cause pain, what should they do then?
“Doing them makes it sore, is that ok?”
“They’ve said in the sheet that the pain begins to settle after about 2 weeks, but doing the exercises makes it sore again so…”
“Should I keep hurting it?”
“Is that maybe making it worse, better?”
By the time she came to see me 3 1/2 months later, her range of movement was still very poor and she was unable to lift a full coffee cup. As a normally very active person, she was feeling very frustrated and knew that her confidence was low - she was now even nervous of going out, in case she hurt her arm further.
So how did we effect this level of improvement in just 1 week?
Education & Reassurance. Exercise modification. Hands-On Treatment. Patient Commitment.
Education and Reassurance
I have known this lady a long time. Although not a regular visitor to my clinic I seem to have fully resolved each issue that she has come in with so, the patient's expectations were already there that I would be able to help with this new issue.
I began by going over a 'normal' or expected length of time for a bone to heal.
It does say this in the sheet she was given but, because the patient was still in pain and unable to do the exercises, she didn’t know if it still applied to her. Plus, I feel that the patient was not prone to believe anything that she had been told/given due to her experience in A&E and the fact that there was no follow up for her to ask questions.
Plus (again!) I defy anyone to remember lots of information whilst they are in extreme pain!
So - a Biology Lesson !
A broken bone will usually heal within 6-12 weeks.
However, a lot of factors will influence this length of time e.g. age of patient, the bone that is broken (a leg bone, the femur, will take longer than a small bone in the hand) whether they smoke or not and how much soft tissue happened at the injury site too.
As her fracture occurred 15 weeks ago, the bone has most likely healed (although only an X-ray would confirm this) and the residual issues that she was experiencing were most likely caused by soft tissue issues - therefore I should be able to help.
The paper, “Fracture Healing in the Elderly” highlights reasons for delayed non-union of a broken bone:
The normal healing time of a fracture varies from 4 weeks to more than 16 weeks depending on the location, the mechanism of injury, and the degree of soft tissue disruption.
Increased age appears to be a risk factor for delayed union or non-union.
The use of non-steroidal anti-inflammatory drugs* and smoking put the patient at greatest risk of these complications.
Therapies such as ultrasound can minimize the risk of delayed union or non-union.
*NSAIDs
“Non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used in both inpatient and outpatient settings to relieve pain. NSAIDs act as an inhibitor of cyclooxygenase, which is involved in the production of pro-inflammatory prostaglandins. These prostaglandins are known to play a role in the regulation of bone formation [40]. By limiting the production of these important signalling molecules, NSAIDs may cause a delay in the formation of new bone during fracture healing”
Teaching the patient the expected length of time for a bone to heal, can go a long a way in managing a patient's expectations and reducing their frustration and fear.
Also, as she had not used anti-inflammatory medication and is not a smoker, we would expect her bone to have healed.
I could tell that this was reassuring for her to hear this and could visibly see her start to relax. (& smile!)
Education and reassurance = happier, more relaxed and less fearful patient.
Exercise Modification
Now obviously, this patient couldn't do the exercises that she had been given, when she was given them - she had a broken arm and I defy anyone to remember how to do an exercise that they've been shown once, 2 months earlier.
Patients often forget what they’ve been taught by the time they get home, ne’er mind 2 months later!
So we went over the ones from her NHS sheet: removing one that was too painful for her, currently and modifying another. So 1 out of the 3 was right for the patient at this point in her healing process.
I always ask the patient to show me the exercises that they've been given elsewhere, as well as ones that I have given.
Sometimes, what a patient has been taught and what they’ve remembered are poles apart (it can be quite fascinating too - the inventiveness!)
Sometimes, I see it as a personal challenge to work out what the original exercise was …..
Just because a patient executes a very weird looking exercise, does not necessarily mean that this is what a therapist has given them!
So don't tut and criticise the previous person.
Even if the exercise is taught well and, is the correct exercise for the patient, what the patient understands and what they remember of the move, even the next day, can be very, very different.
Hands-On Treatment
In the 1st session, the patient's level of pain was too great for any soft tissue work, however this is where craniosacral and myofascial techniques are hugely beneficial.
We did approx 15-20 minutes of gentle hands-on work which helped the patient to understand just how much she was tensing her shoulder - and a tense shoulder will never relax and heal.
Result?
Merely 1 week later the range of motion was vastly improved, the pain had decreased by at least 50% and we have one much happier lady.
Session 2 - 1 week later
We went over her exercises again - all were being executed correctly, and she had done them every day. Gold star pupil!
As her pain level was greatly reduced, I was able to do more hands-on work and treated the rotator cuff muscles with massage techniques, and craniosacral therapy. We were also able to add back in 1 of the original exercises.
Patient Commitment
She did her modified exercises every day.
She didn't add anything else in nor change the exercises.
Because she felt heard, and understood the healing process better, she was less frustrated and fearful of doing further damamge or at least delaying the healing process.
Result!
Takeaways
Reassurance is often an vital but overlooked part of rehab - especially in females and the elderly (males tend to need more ‘reigning in’ than encouragement as they think they can do more than they acually can. (Apologies for the generalisation, it’s my experience from 30 years working in rehab)
If this lady had not known me, if she had not previously had successful treatments, would she have come for help with this issue?
How many other patients are there who cannot afford to pay for private treatment?
How many other patients are there in the UK who are left with severely compromised levels of mobility?
How many other patients are there who go on to develop other issues due to this compromise;
- fear of going out (especially in the older population)?
- inability to maintain an active healthy lifestyle?
- living with chronic pain
When all that was needed, as this lady has shown, was 1 timely and adequate appointment to make a full recovery.
The NHS is under a huge amount of pressure. Not enough staff, money nor time.
I have seen and have experienced, the rushed appointments as they have to move through 100’s of patients in a day.
However.
If this lady had not already known me, or had the fiancial ability to pay for treatment with me, how many NHS appointments might she have taken up?
GP appointments for more painkillers?
Physiotherapy appointments when their lists can be months long?
Or maybe she wouldn’t have ‘bothered’ the NHS whilst her lifestyle beame smaller and smaller?
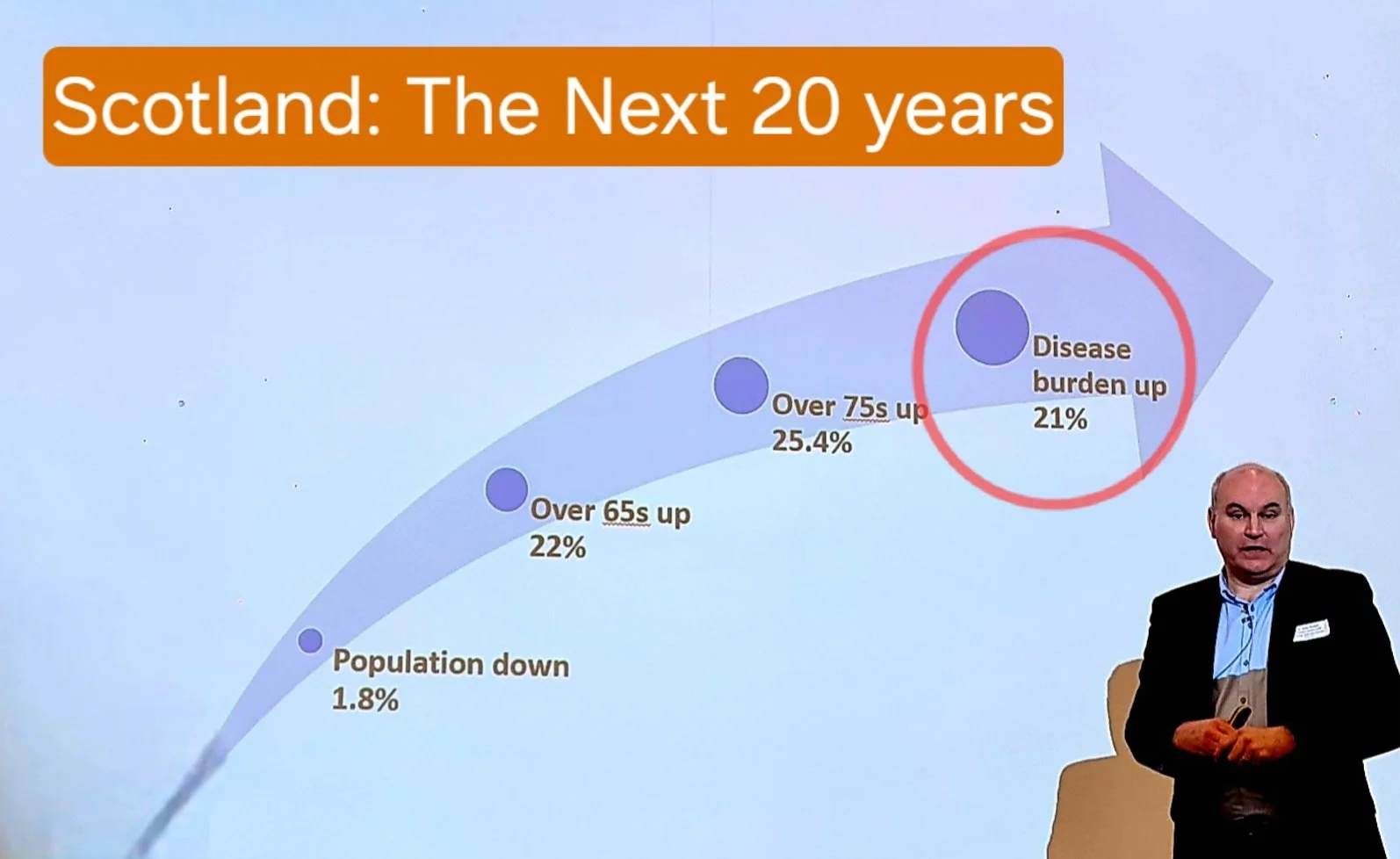
Dr. John Harden, Deputy National Clinical Director, Scottish Govt. presenting at the
Heart Disease Action Plan Conference, 24/04/2024.
If you think the NHS is struggling now, what’s it going to be like in 20 years time?
Attitudes and beliefs from politicians, medical staff and patients alike are going to have to undergo a radical change to ensure that safe and timely treatment is available for those who are most in need.
* Jill is a Clinical Massage Therapist, practising Sports and Rehab therapy, clinical massage and craniosacral therapy.
* She is on the CNHC (Complementary and Natural Healthcare Council) register, the independent UK regulator for complementary healthcare practitioners.
* She is insured to offer; massage, sports therapy & rehabilitation, craniosacral therapy, exercise instruction.
* She has spent 25+ years working within the health & fitness industry both as a teacher and physical therapist.
If you are in Edinburgh you can book an In Clinic appointment below.
Online appointments are also available for those unable to travel or who live further away.